
Cubital Tunnel Syndrome
Cubital Tunnel Syndrome is a problem characterized by an ill-defined ache at the elbow accompanied usually with forearm and numbness in the little-finger side of the hand. The word "cubital" is Latin for "elbow." It comes from compression of the ulnar nerve at the elbow. The nerve at this place is sometimes called the "funny bone." This is a place where the nerve is just below the skin and just superficial to the bone of the elbow, and it is suseptible to compression.
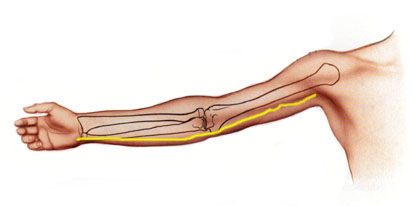
The ulnar nerve is shown in yellow.
At the elbow, the nerve passes from the upper arm, between two bumps of bone, and into the forearm.

Close up view of the ulnar nerve passes behind one bone's bump
(called the medial epicondyle of the humerus) and in front on another
bone's bump (called the olecranon of the ulna). It is vulnerable
to compression here.
Symptoms
The symptoms of cubital tunnel are usually first an odd, poorly defined ache in the elbow. The patient is sure something is wrong, but is not sure where or what. With time, the sensation becomes worse, more defined, and more localized. The patient usually describes an ache at the elbow. Later, the patient may also recognize some numbness in the little and ring fingers.
Physcial Findings
The patient usually has some irritability of the ulnar nerve at the elbow. Light tapping at the "funny bone" causes tingling in the little and ring fingers, plus often an ache along the side of the arm and forearm.
Diagnosis
Diagnosis can usually be made purely on what the patient tells the doctor (the "history") and what the doctor finds on examining the patient (the "physical exam"). Occasionally a nerve conduction test (NCT), sometimes incorrectly called an "EMG" (which stands for "electromyogram", which is Latin for electrical test of the muscle"). Sometimes a NCT is only obtained when surgery is being considered.
Treatment
The treatment starts with the diagnosis. Next comes patient education (which is what this webpage is all about) and activity modification. Full elbow flexion, sustained elbow flexion, and leaning on the elbow all can make the ache and/or numbness worse. Sometimes, if the patient tends to sleep with a fully flexed elbow, loosely wrapping a towel around the elbow and holding it with a safety pin can help prevent full flexion while they are asleep. Sometimes a splint can be made, if the towel treatment does not work out. Most patients can be successfully managed with activity modification, but it takes patience, often on the level of six months.
Sometimes injections are used, but there is not much room here and injections are only occasionally used.
Surgery can sometimes be needed. In surgery, the ligament which is compressing the nerve is released.
Dr. Charles Eaton, an excellent Orthopedic Hand Surgeon in Florida, and a friend: Cubital Tunnel. Once you go to this page, select "Alphabetical List" and then "cubital tunnel".
eMedicine is an online information resourse for physicians. The material is written by physicians, with date of last update, who reviewed it, etc. I know one of the co-authors (Dr. Andy Palmer) and reviewed the material on Sept 29, 2008. I found it accurate. Cubital Tunnel
| Would you like to search the medical library of the National Library of Medicine for scientific papers on this topic? Just click on the Pub - Med image: | |
| Remember the admonition from the Patient Education Links Page: the Internet has a lot of information, much of it incorrect. I have reviewed the sites that I have linked to, and have only linked to sites when I personally know the surgeon who posted it, or am a member of the organization that posted it. However, I may not agree with all that is on that site, and it may have changed since I reviewed it. If any of the information is not consistent with what I have told you, please download the material and bring it in. | |