
![]()
Kienböck's Disease
Kienböck’s Disease
Kienböck disease is a condition in which a one of the small bones of the hand near the wrist called the lunate dies. We don't know what causes it. Although we think of a bone as what is left on our plate after we have a fried chicken dinner, that bone is no more like your bones than fried liver and onions is like your liver. Bone is a living tissue that grows and changes, and it requires a regular supply of blood for nourishment. If the blood supply to a bone stops, the bone can die, a condition known as osteonecrosis ("osteo" = bone and "necrosis" = death, that is, death of bone). Kienböck's disease is osteonecrosis of the lunate. It usually affects the dominant wrist of men aged 20-40 years, but can effect women, but usually later than in men. The true natural history (what happens if we do not treat it) of this condition is not well understood. Not only do we not know what causes it, we do not know why some get better by themselves and some get worse. We don't even know how many have minimal symptoms and get better by themselves, as doctors usually only see a patient after the symptoms are pretty bad. As you can imagine, this has hampered the determination of the ideal treatment. In addition, as with many conditions that affect the wrist, the patient's pain does not necessarily correlate well with the radiographic appearance: some people with almost normal xrays hurt a lot, some with bad xrays hardly hurt at all.
{kind=link}
(Note: the little "ö" is used in spelling the name of this condition because the disease was first described by a Viennese radiologist named Robert Kienböck, and that is how his name is spelled in English. Just thought you might want to know.)
Signs and Symptoms
Many people with Kienböck’s disease think they have a sprained wrist at first. They may have experienced some form of trauma to the wrist, such as a fall. This type of trauma can disrupt the blood flow to the lunate. In most people, two vessels supply blood to the lunate, but in some people there is only one source. Our best guess is that this puts them at greater risk for developing the disease (but as you can understand, we can't do an experiment and prove this!) As the disease progresses, other signs and symptoms may start, including:
- A painful and sometimes swollen wrist
- Limited range of motion in the affected wrist (stiffness)
- Decreased grip strength in the hand
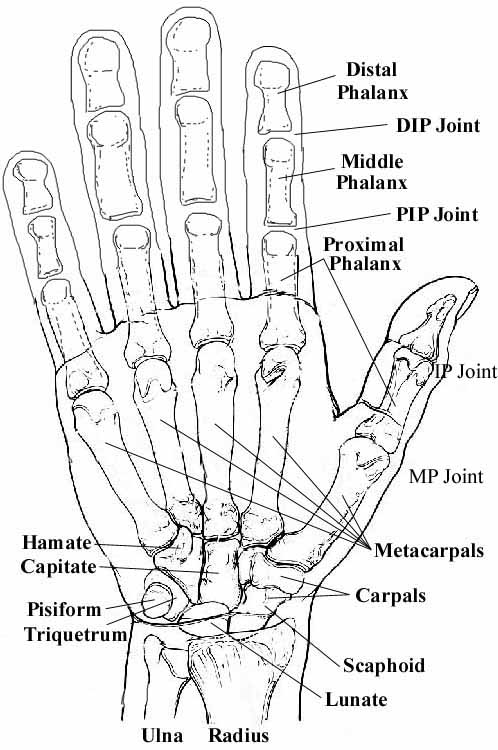
- Tenderness directly over the lunate (on the top of the hand -about the middle of the wrist)
- Pain or difficulty in turning the hand upward
However, as you can see, these things also can occur with many other things, so they are not very specific.
Stages of Disease
Kienböck’s disease follows a specific progressive pattern through five stages.
Stage 0: Symptoms are similar to those of a wrist sprain. X-rays are normal, magnetic resonance imaging (MRI) is normal. (We only know this stage retrospectively, that is, later down the road, when more symptoms occur and more xrays or MRI's are done.)
Stage I: Symptoms are similar to those of a wrist sprain. X-rays may be normal or show a line indicating a possible fracture. Magnetic resonance imaging (MRI) may also be helpful in making the diagnosis in this early stage.
Stage II: The lunate bone begins to harden. On an X-ray, it may appear brighter or whiter than the surrounding bones. These changes indicate that the bone is dying. Either an MRI or a computed tomography (CT) scan may be used to assess the condition of the bone. Recurrent pain, swelling and wrist tenderness are common.
Stage III: The dead bone begins to collapse and break into pieces. The surrounding bones may begin to shift position. Patients experience increasing pain, weakness in gripping, and limited motion. Stage III is broken down into IIIa (no fixed scaphoid rotation) and IIIb (fixed scaphoid rotation).
Stage IV: The surfaces of adjoining bones are affected, resulting in arthritis of the wrist.
Diagnosis
Diagnosis is usually based on a suggestive history and physical exam, then xrays or MRI. In its early stages, Kienböck’s disease may be difficult to diagnose because the symptoms are so similar to those of a sprained wrist. Even X-rays of the wrist may appear normal.
 |
| This is an xray with a patient who has Kienböck’s. Note the lunate has the appearance of being a bit whiter than the other carpal bones, and also has a lucent cyst. |
 |
| This is an MRI of a patient's wrist with Kienböck's Disease. The white bone in the middle is the lunate. Note that the other bones have a darker, greyish color. This lunate is dead. |
Treatment
Treatment is not well-defined, because the natural history (see above) is not well known. However, this is what has worked best:
Medical therapy: Treatment is primarily directed by the level of symptoms. The primary methods of non-operative treatment are immobilization and anti-inflammatory medications. Because our best understanding of the disease is that it is related to loss of blood supply to the lunate, and because we know some patients can be cured if we can just avoid trauma and collapse, this is our first choice in the earlier stages. Younger patients tend to have a better ability to re-establish blood flow to various areas, so in a very young patient, we almost always start with this approach, especially if the disease is early, in hopes of allowing revascularization of the lunate and prevention of disease progression.
Surgical therapy: Surgery is reserved for more advanced disease. Although there is no cure, there are several surgical options for treating the more advanced stages of Kienböck’s disease. The number of options is a bit confusing, so hang in there. The right procedure for you will depend on several factors, including disease progression, your personal activity levels and goals and my experience with various procedures. We will need to discuss this several times. The two most important pieces of information are the stage of your disease and the presence or absence of ulnar variance (the length of the ulna to the length of the the radius).
{kind=link}
Directly comparing the results of different techniques is difficult because most studies have a fairly small number of patients and short follow-up. However, our experience is that many of the techniques result in very similar rates of good outcomes.
Operative treatment can be classified broadly into six categories, including (1) lunate excision with or without replacement; (2) joint-leveling procedures; (3) intercarpal fusions; (4) revascularization; (5) salvage procedures; and (6) others. Let me explain them, in as simple English as the complex problem allows:
- Remove the lunate (the medical term for this is "excision") with or without replacement
- Remove only the dead lunate ("simple lunate excision")
- Remove the dead lunate and replace it with some wadded-up tendon ("excision with soft-tissue replacement", usually fascial or palmaris longus tendon)
Joint-leveling Procedures
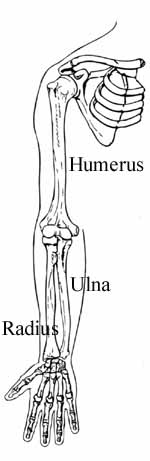
If the bones of the lower arm are uneven in length, a "joint leveling" procedure (shortening the longer bone or lengthening the shorter bone) has been done. Bones can be made longer with bone grafts, or shortened by removing a section of the bone. This reduces the compressive forces on the lunate and seems to halt progression of the disease. Forces on the lunate, caused by using the hand forcefully, are thought to flatten down the lunate, advancing the stage of the disease. This collapsing force can be reduced by 70% with an appropriate radial shortening or ulnar lengthening. Currently, radial shortening with a 3.5-mm metal plate is preferred over ulnar lengthening, as there is a lower complication rate and similar good outcomes. In patients with neutral or positive ulnar variance, shortening the radius is a poor idea. In this clinical situation, radial wedge osteotomies designed to decrease the radial inclination have been proposed. If the lunate is severely collapsed or fragmented, it can be removed. The two bones on either side of it are also removed. This procedure is called a proximal row carpectomy and will relieve pain while maintaining partial wrist motion.
Intercarpal Fusions
Another way to ease pressure on the lunate is to remove some of the wrist bone joints and make them grow together into one or more bigger bones. This is called a fusion. If you make all of the bones grow together, it is called a complete fusion. Usually, we only do some of the bones, this is called a partial fusion. However, this approach may or may not improve range of motion, depending on whether the fusion is complete or partial, and on the stage of the disease, and on the amount of motion you started with. If the disease has progressed to severe arthritis of the wrist, fusing the bones will reduce pain and help maintain function, although motion is limited. A variety of intercarpal fusions for the treatment of Kienbock disease have been used. The goal is to reduce forces on the lunate, crushing it down, and, in procedures that involve the scaphoid, to correct and maintain proper scaphoid position.
Of the limited intercarpal fusions used, the greatest experience has been with scaphotrapeziotrapezoid (STT) (triscaphe) fusion. STT arthrodesis (fusion) decreases lunate compression forcesby shifting it to the radioscaphoid joint. This can cause later problems. STT fusion in a cadaver model was found to have similar strain reduction to that of joint-leveling procedures but had greater loss of motion. The use of STT fusion has waned in recent years due to complications and longer-term follow-up revealing decreased success rates.
Scaphocapitate (SC) fusion has been used by some surgeons. Biomechanically, this fusion has been shown to reduce compressive forces at the radiolunate joint by about 10%. Some surgeons prefer this fusion because it requires only one fusion site and is technically easier to perform.
At the present time, intercarpal fusions more likely are reserved for patients with neutral or positive ulnar variance in whom a joint-leveling procedure is a bad idea.
Revascularization
In some cases, returning the blood supply to the bone (revascularization) may be possible. This procedure uses a bone graft from the bone of the lower arm with a very little artery attached. This is called, in medical terms, a vascularized bone pedicle. I want you to get used to this term, as I will use it when I discuss your options. Results with the use of pedicled distal radius grafts have shown improved grip strengths and progressive MRI evidence of revascularization over an 18 to 36 month period (Mazur). Revascularization techniques may also be combined with other previously mentioned approaches, particularly it may be combined with an external fixator, a metal device that helps relieve pressure on the lunate and preserve the spacing between bones. Revascularization is especially attractive for the young patient with ulnar neutral or positive variance in whom a radial shortening is not an option and in one who wishes to avoid an intercarpal fusion and resultant loss of motion.
What to do if all else fails
Salvage procedures are what we call the surgeries that are used when all else fails. One procedure that has worked rather well, despite how destructive it sounds: cut out three of the little bones of the wrist (scaphoid, lunate, triquetrum.) This is called a proximal row carpectomy (PRC). It has been shown to provide relatively good results in Kienbock disease, both by several studies published in the hand surgery literature as well as by a several very good friends of mine locally, who are in a hand surgery study group I have run for over 12 years. Our experience with a PRC is also supported by the fact that it works well for other wrist problems, so we have more experience with this surgical approach than with many of the others, which are only used for the relatively rare condition of Kienbock's. Complete wrist fusion (arthrodesis) is the final option for patients with global wrist degeneration. Arthrodesis can be achieved successfully following a failed PRC. It always works to stop the pain, and although the patient cannot do wrist flexion and extension, they usually have increased function in their wrist because the pain is gone. Talk to me about this, as this is rather complex, but very well documented and understood. I did some of the research that established this concept.
| Would you like to search the medical library of the National Library of Medicine for scientific papers on this topic? Just click on the Pub - Med image: | |
| Remember the admonition from the Patient Education Links Page: the Internet has a lot of information, much of it incorrect. I have reviewed the sites that I have linked to, and have only linked to sites when I personally know the surgeon who posted it, or am a member of the organization that posted it. However, I may not agree with all that is on that site, and it may have changed since I reviewed it. If any of the information is not consistent with what I have told you, please download the material and bring it in. | |