
Trigger Finger
What is trigger finger or trigger thumb?
Trigger finger and trigger thumb are some of the most common conditions I treat in my office. It is due to a swollen part of the tendon at the base of the digit. It can cause a painful popping and clicking in the finger or thumb as the patient flexes or extends the digit. It is very common for this to occur just when you wake up in the morning. If the condition is not treated, it will commonly worsen to the point that the patient cannot fully straighten the finger (or sometimes cannot flex, although that is less common). The painful popping and clicking is called "triggering" (this is where the name comes from) and the inability to fully straighten is called "locking". To better understand how this happens, look at the illustration below.
The Palm of the Hand
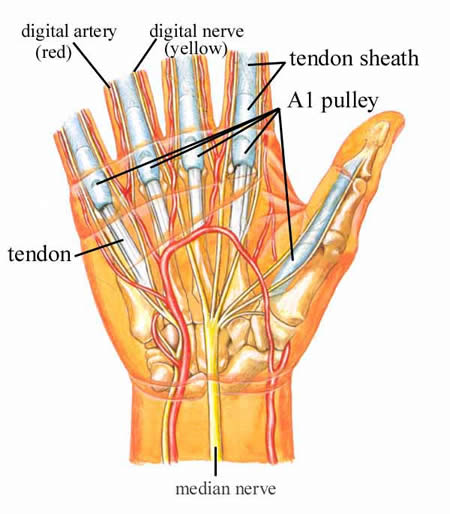
This is a view of the palm side of the hand. The tendons, shown in white, pass into the finger inside a tendon sheath, shown as a slightly bluish-white. This sheath functions to keep the synovial fluid (the "tendon oil") around the tendon. The synovial fluid lubricates the tendon as it moves back and forth in the finger. The beginning of the sheath is called the A1 pulley. Note the digital (finger) artery and nerve. They are very close to the pulleys. The illustration below shows an enlarged view of the pulley system.
Enlarged View of the Pulley System
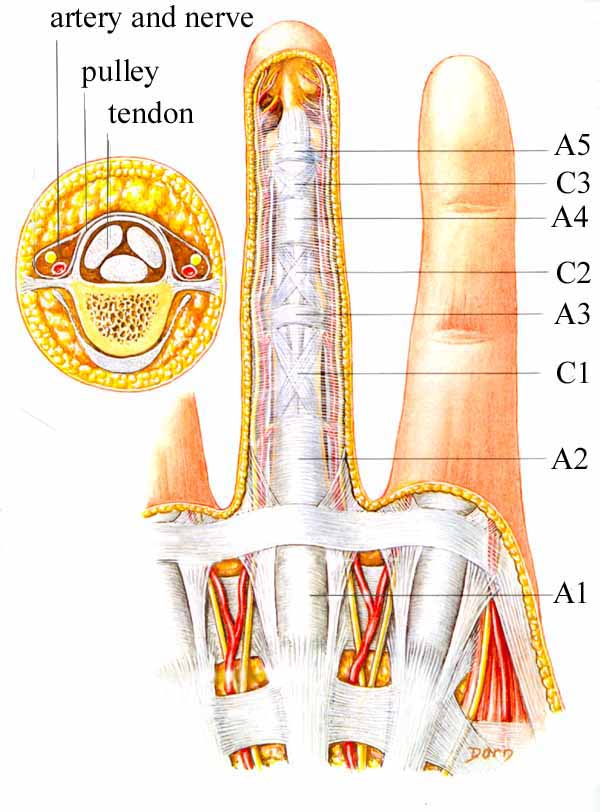
This illustration shows the tendon sheath, and shows how it has some thicker regions that are divided into named structures called pulleys. The A1 region is the one that gets involved in trigger finger. There is a similar division, but much simpler, in the thumb. The purpose of the pulleys is to keep the tendons close to the bone (see the smaller illustration above, to the left). As the finger bends (flexes), the pulleys prevent the tendons from sagging away from the bone. In trigger finger, there is some swelling of the tendon, due to a variety of factors, mostly processes of aging. The swollen part of the tendon "pops" under the A1 pulley, causing the finger to "pop" or not bend smoothly. Often the patient thinks it is the joint that is popping, but it is the tendon that moves that joint that is popping.
What causes trigger finger?
We do not know exactly what causes trigger finger, but we do know some things. The tendon is subjected to significant forces at the A1 pulley, which is where trigger finger occurs. Trigger fingers show changes in the substance of both the tendon and the pulley called "fibrocartilaginous metaplasia", which means that some of the cells change into cells that have the characteristics of cartilage cells such as those found in intervertebral disks. The cells show an increase in both the size of the cells and the number of cells. The smooth gliding layer of the tendon and the pulley change, with fraying and disintegration of the surface. We do not see these high forces or cellular changes in other areas of the flexor tendons, therefore we feel that these changes must be related to the disease called trigger finger. (Trigger Digits: Diagnosis and Treatment, by Miguel J. Saldana, MD; Journal of the AAOS, July/August, 2001, pages 246-252).
In addition, the molecules of the collagen (collagen makes up about 95% of the substance of a tendon) degrade and break up. The degredation products of the collagen, called "mucinous degeneration", accumulate within the tendon, enlarging the area (see illustration, below). This in part creates the bump or swelling of the tendon. This seems to be a natural part of aging (like grey hair and wrinkles) and is not a sign of disease or overuse. That is, we do not see trigger nodules more commonly in people who do heavy manual labor for a living and we do not see it more commonly in the dominant hand, even though we all use our dominant hand much more than our non-dominant hand. Trigger nodules are most commonly seen in adults of middle age, especially post-menopausal women and men of a similar age.
 |
 |
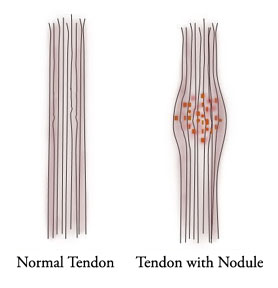
| The normal tendon is composed of very parallel strands of collagen. The trigger nodule has degredation products of collagen accumulating within the strands of collagen inside the tendon, creating a fat place or "nodule" in the tendon. (Illustration by Dr. Nelson) | The nodule inside the tendon can grow so big that it cannot pass under the pulley, shown in green. |
What are the symptoms of trigger finger?
The hallmarks of trigger finger is painful popping of the digit and pain in the palm at the A1 pulley level. The popping is usually worse in the morning when you first get up, but as the problem progresses, it can pop all the time. When it is really bad, the bump in the tendon cannot pass under the pulley and the finger is "locked", that is, it cannot straighten (or bend, if it is stuck out straight).
Who gets trigger finger?
Many people think trigger finger should come from a long history of hard work, but hard labor does not seem to be very related. It can come from an episode of overuse, but is usually not associated with any period of heavy use. It usually comes on gradually, and typically comes in our 40's, 50's, and 60's. It is about two to three times more common in women than in men, and the fourth finger is the most often involved. It is common for patients to get it in more than one finger. If they do, it is often either the same finger in both hands, or two adjacent fingers. I have only had one patient who had it in all 10 fingers, and he was a 60 year old who played handball. I think if you are 60 and go around whacking things with your palm, you should expect to get problems! Most patients will get it in only one or two fingers.
How is trigger finger diagnosed?
The diagnosis is made by listening to the patient and by examining the patient. Most patients will have a history of painful clicking and popping, without any history of trauma. There will be a painful nodule in the palm, exactly at the A1 pulley location.
How is trigger finger treated?
Here is an outline of my treatment for hand problems in general. I will show you how it is tailored to trigger finger.
Outline of My Treatment for Hand Problems in General
1 Diagnosis
2 Patient education
3 Activity modification
4 Anti-inflammatory medication
5 Splints
6 Hand therapy
7 Steroid injection
8 Surgery
You start out with diagnosis. In the case of trigger finger, the making of the diagnosis is usually quite simple. The next step is very important: patient education; that is why I wrote this page (on a Thanksgiving holiday!) and why I have referred you to this page.
The third step in my general treatment regimen for all hand problems is activity modification. This step does not really apply much to trigger finger. It is usually not due to overuse, and in the case of my handball-playing patient, he wanted to keep playing, and I don't blame him. On to the next step!
The fourth step in my general treatment regimen for all hand problems is anti-inflammatory medication. This usually does not help in the treatment of trigger fingers. It is not strictly an inflammatory condition, since the changes are not just the changes of inflammation, but of fibrocartilangenous metaplasia (see section above for explanation).
The fifth step in my general treatment regimen for all hand problems is splints. While they will work as long as you wear the splints, you will not be able to do anything with your hand. If the trigger digit was minimally symptomatic and you happened to do something that made your hand swell, a temporary splint may help. However, splints usually are not a part of the treatment of trigger finger.
The sixth step in my general treatment regimen for all hand problems is hand therapy. While I use a lot of hand therapy in my practice, there is not much that hand therapy can offer this condition.
The seventh step in my general treatment regimen for all hand problems is steroid injection, and this is a great way to treat trigger fingers. About 50% of all trigger fingers will be completely resolved with injections, although it may take more than one. It is not a good idea, in general, to give more than three injections in any one location in the body, as it can cause some collagen degeneration and tendon rupture (see image below). You can have three in each involved finger, but not more than three in any one finger. If a finger has been locked, the injection will often resolve the locking, but it probably will not be completely effective in resolving the problem, and you are more likely to proceed to the next step.

Tendon ruptured by too many steroid injections for trigger finger
The final step is surgery. About 50% of trigger fingers go on to surgery. The longer you waited to come see me, the greater the chance that you will need surgery. There are two surgical techniques: percutaneous needle release and open release.
Percutaneous Release
"Percutaneous" means through the skin, and the technique involves using the tip of the needle as a mini scalpel. The doctor inserts a needle through the skin at the level of the A1 pulley and using the tip of the needle, sweeps it back and forth, cutting the pulley. The advantage of this technique is that you do not have an open incision, the procedure is done in the office (you do not have it done in an operating room), and there is no incision to heal. The tendon will be a bit tender for a few days to a few weeks. The disadvantage is that this is a blind procedure: I am not able to see the pulley or the tendon. I will not be able to guarantee that I can successfully release the pulley and you may still have to have it released in an operating room; this has not happened yet, but it could. I am just mentioning it so that you are aware of the possibility. There will be some level of tendon damage from the tip of the needle. This "damage" is very limited and the needle cuts the tendon in line with its fibers, so it is just as strong immediately after surgery as it was before. There is some risk of injuring the nerves or arteries, since it is a blind procedure, but this should be rare: less than 1% chance.
Standard Open Release
The standard technique, called an Open Release, is to make a 3/4 inch incision directly over the A1 pulley, which is only about 1/4 inch below the skin. The pulley is released under direct vision and the skin is sutured closed. Of all the surgeries I do, this is the simplest. It is out-patient surgery (that is, you don't stay overnight in the hospital). You don't even have to eat the hospital food! (Although I rather like the Marin General Hospital food, and think that they do a good job.)
You come in about 1 hour before surgery is scheduled, the procedure takes about 15 minutes, and you are out about one hour later. The anesthesia is usually only a local block (don't worry about the surgery hurting: I have more medicine than you have nerves!), supplemented with a little IV sedation. You just tell the anesthesiologist how awake you want to be (or don't want to be!), and they can adjust the amount of sedation to suit you. We are using a new generation of anesthetic, and you will not feel like you have been run over by a truck. Most patients say they felt like themselves within minutes after the surgery. The post-operative pain is described by most of the patients as minimal (see my pain study). Most patients will be using their hand the next day, but you will be using it very gently. There are usually no sutures to be removed (I place absorbing sutures inside, so you never see them), and you change from a small dressing to a Band-Aid at three days.
The risks of surgery are minimal, but not zero. Infection, failure to relieve the triggering, recurrence of triggering, or damage to local structures are the main complications, and should be at about the 1% level. I have not yet had a complication during the surgery. I have had one get infected, 3 months after surgery, but this patient never kept any of her followup appointments; the wound was draining but she did not think anything of it. I am always careful, but complications can happen, even with the best of care.
Both procedures are not appropriate for all patients. I would like to discuss them with you in the office during your visit.
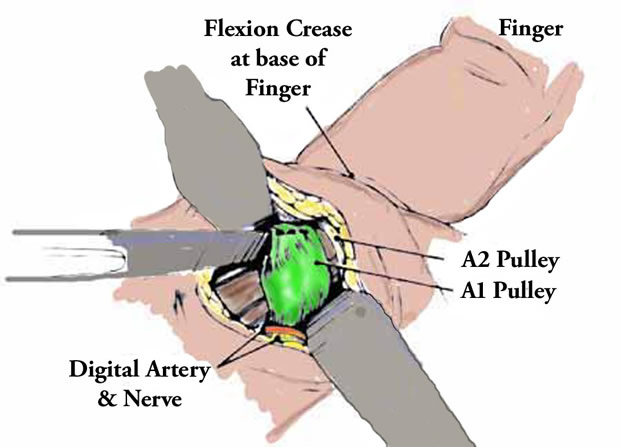
A Diagram of the Surgical Procedure
Here you see two retractors (the grey blobs) holding the incision open; the pulley (in green) is being cut by the scalpel (grey thing coming in from the left). Digital artery and nerve are identified at bottom left.
What Can I Expect After Surgery
Predicting the future is difficult, but I can tell you what is typical for most cases and for most patients. All the sutures will be under the skin, like a Hollywood movie star's plastic surgery, so you will not see the sutures and there will not be any sutures to be removed. Nice, eh? You will have a small dressing on your palm, but not on your wrist or finger. You can use your hand gently, even the day of surgery, but it will be numb for 8 to 36 hours (this is to prevent post-operative pain, see my page on post operative pain). The dressing must be kept dry (see post operative instructions ) for five days, so use a plastic bag to shower. On the third or fourth day, you can take the dressing off and place a bandaid. Two days later, you can get rid of the bandaid and get it wet in the shower. You can get it wet in dishwater or a hot tub at 7 days after surgery. Use your hand gently, but it is exceedingly rare for someone to be able to open their incision (has happened four times in 20 years, but only due to falling on the hand!) Gradually increase your activities. It is hard to predict exactly how quickly each patient will return to activities, as there are many variables, including the exact procedure performed, how active the patient normally is, how much discomfort each patient will tolerate before they limit their activities, etc. However, many people will drive the next day, type in a day or two, resume serious keyboard use in a week or two, play tennis in 1-3 weeks, return to paperwork jobs in 1-2 weeks, return to manual labor jobs at 3-4 weeks. I will discuss the particulars of your surgery and recovery with you in the office.
Click here if you want to read what other patients have written about their experience with trigger finger surgery.
The American Society for Surgery of the Hand has a YouTube video on trigger finger.
American Society for Surgery of the Hand: Trigger Finger Brochure. .
Dr. Charles Eaton, an excellent Orthopedic Hand Surgeon in Florida, and a friend: Trigger Finger. Once you go to this page, select "Alphabetical List" and then "trigger finger."
| Would you like to search the medical library of the National Library of Medicine for scientific papers on this topic? Just click on the Pub - Med image: | |
| Remember the admonition from the Patient Education Links Page: the Internet has a lot of information, much of it incorrect. I have reviewed the sites that I have linked to, and have only linked to sites when I personally know the surgeon who posted it, or am a member of the organization that posted it. However, I may not agree with all that is on that site, and it may have changed since I reviewed it. If any of the information is not consistent with what I have told you, please download the material and bring it in. | |