
Tennis Elbow
Tennis Elbow is a terrible name! The reason is it a terrible name is that is it wrong in both words! It is usually is not from tennis and the problem is not what you do with your elbow! Although the pain is at the elbow, the problem is what you do with your wrist and fingers. Its medical name is "lateral epicondylitis", which is more correct but still misleading. Patient education is probably more important in tennis elbow than in almost any other condition I treat. If you don't teach yourself about your condition, you will probably continue to injure yourself. If you learn about the condition, modify how you use your arm and hand, about 92% of people can avoid surgery. Let's go!
What is Tennis Elbow?
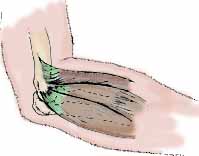
Tennis elbow is a type of painful tendinitis. More precisely, lateral epicondylitis is due to a tear and resulting inflammation (that is why the name ends in "-itis", which means inflammation) of the collagen fibers that attach the forearm extensor muscles to the outside of the elbow (which called the lateral [or outside] epicondyle [or end of the bone]). This is diagrammed in the illustration below. The extensor muscles extend (lift) the wrist and hand. The muscles also have to contract when you make a firm grip, in order to extend the wrist and allow you to close your fingers forcefully. (Just try to make a firm grip when your are fully flexing your wrist!) The muscle which is usually the most irritated is the the extensor carpi radialis brevis. This name is just Latin that means "the short muscle that extends the wrist". It is the middle muscle in the diagram below. The collagen fibers that connect the muscle to the bone are a combination of tendinous fibers and some specialized fibers called Sharpie's fibers (both are shown in green in the diagram below). In the elbow, the common origin is well-developed and looks like a flat strap of gristle.
Forceful muscle contractions in the common wrist extensors may result in pain where these fibers attach to the bone on the outside of the elbow or along the muscles in the forearm. Pain is usually aggravated by any forceful gripping and lifting with the hand in certain positions (palm down, called pronation). Pain is usually more noticeable during or after stressful use of the arm. There may be swelling on the side of the elbow, but this is usually minimal. In severe cases, lifting and grasping even light things may be painful.
The name "tennis elbow" came from the fact that beginners people who take up tennis or other racquet sports sometimes develop this problem from improper playing technique. The condition arises in beginners, who think a backhand is a wrist motion. Experts know that shoulder muscles are larger and stronger than wrist muscles, so they use shoulder muscles for a backhand. Medial epicondylitis or “golfers elbow” is a similar condition that occurs on the inside of the elbow. The condition is quite common in our late 30s and early 40s.
What causes Tennis Elbow?
Although tennis elbow can arise for no obvious reason, the most common situation in which tennis elbow develops is following unaccustomed strenuous activity involving the arm and hand. This could be activities such as using a screwdriver to place a few dozen screws, or scrubbing a floor vigorously. It also commonly develops in people who are increasing their level of activity in work or recreation that requires wrist extension and/or firm grip.
The area of the common origin is hard and pushes against the side of the bone. It does not stretch or easily accommodate swelling, and if irritated by sudden overuse, pressure may build up and cut off the blood supply to the middle of the tendon. The tendon wraps around an area where the bone sticks out, and pressure between this bone and the hard outer layer of tendon may squeeze the inner parts of the tendon like a nutcracker. This can be very painful!
Once the fibers in the common externsor origin are torn, the fibers of origin may not be able to heal unless you rest them, or may heal very slowly over many months if you do not rest them long enough. This slow healing may have to do with decreased circulation in the common extensor tendon, but also because the area is stretched and twisted by normal movement of the elbow, making it hard for irritated areas to rest. If you do not change how you are using your wrist and hand, you continue to injure the common extensor tendon.
Tennis elbow is usually a chronic problem. Patients do not know why their elbow is hurting, so they continue to injure themselves, overusing the extensor muscles of the forearm and tearing the common origin. This sets up a vicious circle of tearing the fibers, some healing (tendinous tissues like Sharpie's fibers heal by scarring), then repeat tearing before the healing has had a chance, and further scarring. A famous researcher in this topic, Dr. Nirschl, called this "unsatisfied scar", which I think is a great name!
What does Tennis Elbow look like at the microscopic level?
If you want to see what your elbow looks like at a microscopic level, as it is torn and heals, click here.
What about a steroid shot?
Many people have heard of steroid injections or know patients who have had a steroid injection for tennis elbow. This has been a standard treatment since a paper on it in 1948. However, as the quality of scientific studies of steroid injections for tennis elbow have improved, it has been found that actuallty, steroid injected PROLONG recovery and DO NOT HELP HEAL tennis elbow. There is sometimes (30% of patients) a temporary improvement, less than a month, but it does not help, they actually hinder recovery. Here is how Dr. David Ring, of Harvard, summarized the scientific data:
"Methods: 7 randomized controlled trials comparing the effect of corticosteroid injection with a placebo injection on symptoms of tennis elbow were included in our analysis.
Results: We found no difference in pain intensity 6 months after injection of corticosteroids or placebo. Pain intensity was slightly, but significantly lower 1 month, but not 3 months after steroid injection. There were no significant differences in grip strength or DASH score at any time point.
Conclusions: A minimum of 3 patients needs to have an injection for 1 to experience slight improvement in pain 1 month after injection. We interpret the weight of evidence to date as suggesting that corticosteroid injections are neither meaningfully palliative, nor disease modifying when used to treat eECRB."
It typically takes 12 months to 18 months for tennis elbow to heal. If you do not change how you use your hand, it will take longer.
What can you do to help youself?
The most important thing to do is first, learn why and how you are hurting yourself (that is what this webpage is about), and then, stop doing it! As I noted at the top of this page, about 92% of tennis elbow can be treated without surgery.
Ice for five to fifteen minutes at a time on the area which is most swollen and tender. After the acute stage has resolved, healing (scar formation) has had a chance to take place, and the scar has matured to the point that it can take some pulling by the muscles, you can start to slowly and gently resume activities.
It is very important that you not overuse your arm while the healing is taking place. If it still hurts, even a little, you are overdoing it! The only way to break the cycle is to rest your arm until the vicious circle is broken.
Sometimes a band wrapped around the forearm near the elbow (tennis elbow strap, also called a counterforce splint, is available at many drug stores) can be used to protect the injured muscles as they are healing. In some cases, the wearing of a wrist splint may be useful for the same purpose. Anti-inflammatory medication, can be taken by mouth. In severe or long-lasting episodes, an injection of steroids into the area may relieve the discomfort. Your hand surgeon may recommend exercises that stretch and strengthen the muscles to help prevent the condition from returning. Some patients respond to additional treatment through therapy. As the condition improves, there is usually a slow return to normal activities. Recurrence of this condition is common.
Exercises should not be performed until the area is no longer swollen and tender. If, during the course of strengthening the muscles and Sharpie's fibers, you experience tenderness and/or pain, STOP! You are starting the vicious circle all over again. Rest until you can do the exercises without pain. Lateral epicondylitis is often a nagging or chronic condition sometimes requiring many months for healing to occur.
If nonsurgical forms of treatment do not eliminate the pain of this condition, surgery may be recommended. I need to discuss with you the surgical treatments for lateral epicondylitis and the possible outcomes.
Injection of Blood
The problem in tennis elbow is a lack of adequate healing. An injection of your own blood can help. Read this article and discuss it with me.
What can a therapist do to help?
The most important thing a therapist can do is to help to teach you about the the anatomy of the area and the mechanism of injury. They can help identify aggravating activities and suggest to you alternative postures. They can provide a forearm strap or wrist brace to help protect the irritated area. They can instruct you in a home program of massage, heat, ice and other treatments aimed at making the area more comfortable. Once you have let the scar tissue mature, they can supervise a set of progressive exercises designed to gradually strengthen and recondition the irritated muscles. Remember, however, even if the therapist has given you exercises to do, STOP if you experience the pain returning.
Tennis elbow is a common problem, so there is a lot written about it. I have based this essay on my own experience and on some of the following:
Dr. Jeff Budoff has an extensice webpage on tennis elbow.
American Society for Surgery of the Hand: Lateral Epicondylitis Patient Education Brochure.
Dr. Charles Eaton, an excellent Orthopedic Hand Surgeon in Florida, and a friend: Tennis Elbow.
| Would you like to search the medical library of the National Library of Medicine for scientific papers on this topic? Just click on the Pub - Med image: | |
| Remember the admonition from the Patient Education Links Page: the Internet has a lot of information, much of it incorrect. I have reviewed the sites that I have linked to, and have only linked to sites when I personally know the surgeon who posted it, or am a member of the organization that posted it. However, I may not agree with all that is on that site, and it may have changed since I reviewed it. If any of the information is not consistent with what I have told you, please download the material and bring it in. | |